
Cognitive Flexibility
Cognitive flexibility is a broad term allied to the concept of control and is used to refer to a person’s ability to switch from one task to another.
Cognitive flexibility (or shifting) is an important function that allows a person to move attention from one stimulus to another in a seamless and efficient manner (P. Anderson, 2008) and is an integral part of the larger attention and working memory systems Opens in new window.
Such shifting can take place in response to environmental stimuli, such as being interrupted, or by cognitively shifting one’s thought process between selecting where one’s attention should be focused.
Implicit in this requirement is the demand to curtail or inhibit Opens in new window one behavior and spontaneously commence another.
Clinically, tests that measure these characteristics typically set up an automatic expectancy or routine of behavior in the patient and then require the patient to shift from that expectancy or routine in an independent manner.
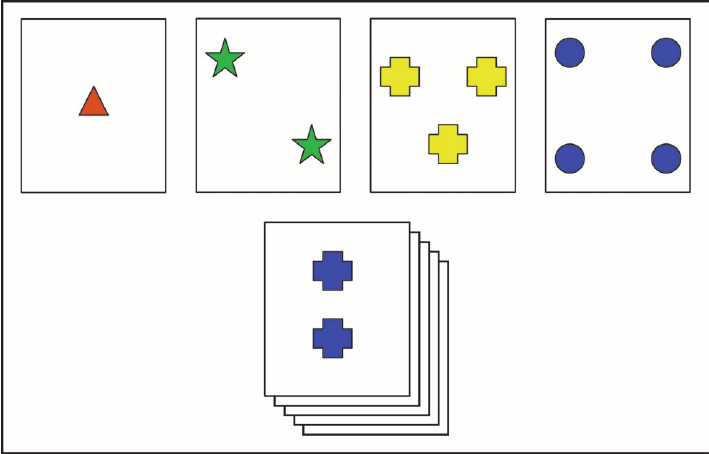
The Wisconsin Card Sorting Test (WCST; Grant & Berg, 1948) is perhaps the most famous of the set-shifting tests. This test provides four target cards incorporating different colors, numbers or shapes, which are placed up in front of the patient (see Figure X-1).
|
| Figure X-1. Credit: ResearchGate Opens in new window | A representation of the Wisconsin Card Sorting Task. The 4 piles (top) differ with respect to color, shape, and numerosity, and subjects must sort test cards (pile below) into these piles via a certain rule. In this case, if the rule were shape, the test card would be placed with the pile of crosses. |
Cards from a pack are placed one at a time underneath one of these four target cards on the basis of a match of either color, number or shape. Initially, only the clinician knows which of these matching strategies is correct.
In a survey, the subject has decided to go for a match according to shape rather than color or number. The clinician will say ‘correct’ or ‘incorrect’ to the subject’s placement, until eventually the subject discovers the correct rule by trial and error. In the easier, perhaps less sensitive, modified version (Nelson, 1976) the patient will be told that the rule has been changed.
In the original version pioneered and first used with patients by Brenda Milner, the examiner changes the rule, e.g. from number to color, without telling the patient. The patient has to work out that this has happened purely by monitoring feedback (i.e. whether their response is designated correct or incorrect by the examiner).
Two main measures, the number of categories (rules) achieved and the number of perseverations, are used from this task. At this point it should be noted that even in the most reliable indicator of frontal dysfunction the perseveration measure is somewhat ambiguous.
Perseveration Opens in new window occurs when a behavior is repeated despite a history of negative feedback. It is therefore in short a non-adaptive repetition of behavior, and although it is often taken as a sign of poor cognitive flexibility this broad description may be misleading.
Perseveration Opens in new window occurs in the WCST when the patient doggedly persists with a previously relevant but now irrelevant rule despite clear indications that the rule has been changed. Thus, they may continue sorting the pack according to color, even though the feedback indicates this is no longer the basis on which the cards should be matched.
While the WCST showed much promise originally, recent studies and reviews have questioned whether this is a diagnostically useful task (Bowden, et al., 1988; Hermann, Wyler, & Richey, 1988; Mountain & Snow, 1993), although careful use of the results of this test may be useful (Stuss et al., 2000).
Components in Cognitive Flexibility Process
The process of cognitive flexibility that underlies the process of set shifting can possibly be broken down into subcomponents. In the event of shifting from one routine behavior to another, the patient may theoretically have to undertake two processes.
First, the original “expected” behavior must be suppressed or inhibited, then the patient must initiate the new response.
Burgess and Shallice (1996) used a paradigm to dissociate these two features in a task that required patients to complete sentences (the Hayling Test).
In their task, the final word in the sentences was missing and subjects were timed as they completed the sentences (an initiation task). Then subjects were asked to do a similar task, only this time they were required to use a word to complete the sentence that was unrelated to the sentence. In the second task the patient needed to suppress or inhibit their natural inclination to complete the sentence.
As predicted, the initiation/completion task was slower in the patients with anterior lesions compared to the posterior lesioned patients. The patients not only slowed up in the suppression task but they also tended to make more errors either by going against instructions by completing the sentence or by using a word that was in some way conceptually related to the sentence.
Although patients with bilateral frontal lesions in this study did poorly on both tasks, some of the patients with unilateral lesions did more poorly on one task compared to the other.
The lack of an association between the performance on these tasks suggested two processes. However, the authors point out that this proposal awaits verification because of other possible interpretations of this finding. Therefore it is possible that a distinction might be made between patients who find initiation more difficult, while others find the inhibition of response more difficult within the process of cognitive flexibility.
Finally, on this topic of cognitive flexibility and control, it should be acknowledge that even without brain damage a person may be poor or good at controlling their own behavior. It is a commonly held clinical view (but to the author’s knowledge, not yet empirically verified) that brain damage to the frontal region may exaggerate the premorbid personality of the patient. For example, if the patient is disinhibited prior to frontal brain damage this aspect of their personality might be exaggerated.
You Might Also Like:
- Barbey, A. K., Colom, R. & Grafman, J. (2013). Architecture of cognitive flexibility revealed by lesion mapping. NeuroImage, 82, 547-554.
- Anderson, S. W., Damasio, H., Jones, R. D., & Tranel, D. (1991). Wisconsin card sorting test performance as a measure of frontal lobe damage. Journal of Clinical Experimental Neurospychology, 13, 909-922.
- Aron, A. R. (2007). The neural basis of inhibition in cognitive control. Neuroscientist, 13, 214-228.
- Aron, A. R. (2011). From reactive to proactive and selective control: Developing a richer model for stopping inappropriate responses. Biological Psychiatry, 69, e55-e68.
